The load that is a person
Most burnout advice assumes the load is something you can negotiate with. Fewer hours. Fewer meetings. A different team. A sabbatical.
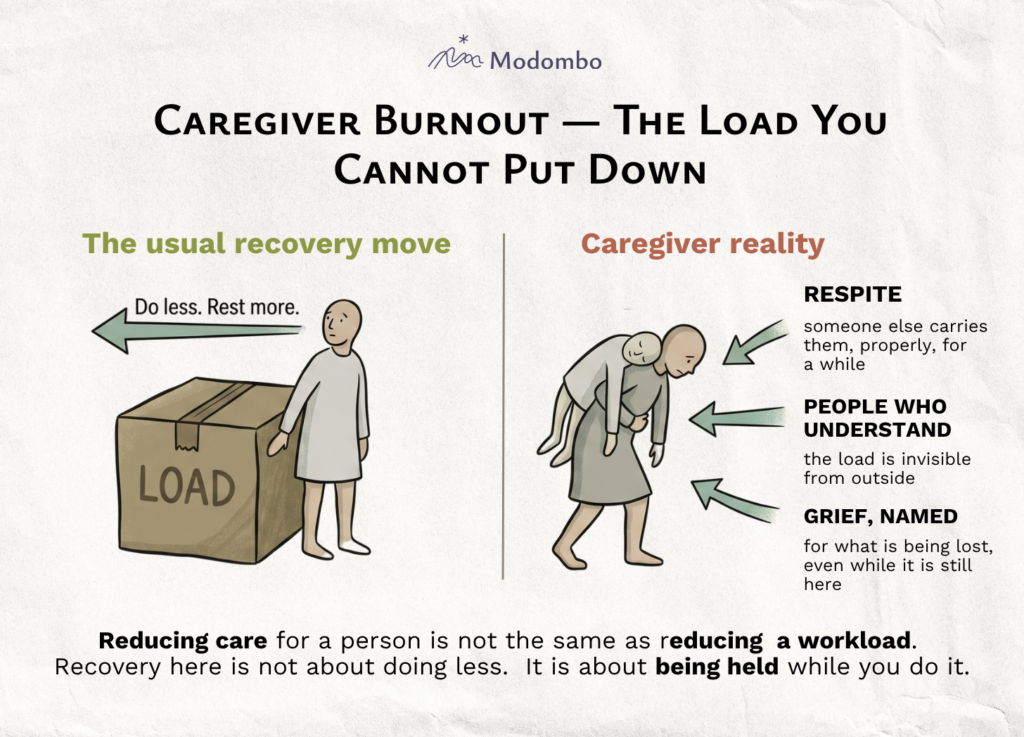
Caregiver burnout breaks that assumption at the root. The load is a child with a disability, an aging parent whose mind is going, a partner with a chronic illness, or, in the professional version, a caseload of patients or clients you cannot unsee once you have seen them. You can change how you carry it. You cannot put it down. “Do less” arrives as advice that quietly means “care less,” which the caregiver is not willing to do and should not be asked to.
How it sounds in the room
- “I haven’t had a thought that wasn’t about their care in months.”
- “When people ask how I am, I don’t know what to answer. It’s not really about me anymore.”
- “I love them. I also resent them. Both are true, and neither one leaves.”
- “I feel guilty when I take an hour for myself. I feel guilty when I don’t.”
For professional caregivers the phrasing shifts: I come home and I can’t listen to my own family. I have no more listening left.
Why the standard advice misses
The usual burnout toolkit assumes the person can shrink the load. Here the load is not a schedule. It is someone’s need, and the need does not pause for your weekend.
Telling a caregiver to “set better boundaries” assumes the boundary is with a colleague. Telling them to “take time off” assumes someone else can step into the role. Sometimes that someone exists. Often they do not, or they exist in theory and arrive with their own fragility. The caregiver reads the advice, recognizes it does not apply to their life, and concludes quietly that burnout resources are written for someone else.
People tell you caregiving is a privilege. Sometimes it is. Sometimes it is just what is happening to you, and the word privilege does not help.
What actually helps
Recovery here is not subtraction. It is closer to scaffolding. Three directions tend to matter more than any advice the caregiver has already seen.
Real respite. Someone else actually holding the load while you are properly off, not on-call from the next room. For domestic caregivers this is often the missing piece: a relative, a paid carer, a respite programme, something that makes the hand-off complete enough that the nervous system can down-regulate. A weekend away while still answering the phone every ninety minutes is not respite. It is commute plus guilt.
What turns respite into recovery is regularity, not size. A weekend off taken once after months of nothing often makes things worse before it makes them better. The moment the load is set down, the underlying despair becomes visible, and the caregiver returns more shaken than rested. What holds is the expectation that the next handover is already on the calendar, in a week or in a month. Daily micro-respite matters too: fifteen minutes of solitude, a walk no one else interrupts. The nervous system needs both rhythms.
People who have done this, or are doing it. The load is invisible from the outside, and most of the caregiver’s social world does not know how to meet them. Groups of other caregivers, formal or informal, tend to matter more than a generic support network, because the conversation does not have to start from scratch each time.
Seeing another caregiver carry a comparable load is often the door-opener. It is what lets a person finally admit, quietly, that they are on the path to burnout, and what gives them permission to take respite seriously, because someone they trust has already done it without the world ending.
Naming the grief that is already running. Caregiving for someone in decline is a rolling loss most people carry without words. Naming it, that you are grieving in stages while the person is still here, does not fix anything, but it stops you from reading ordinary grief symptoms as your own failure.
Those symptoms are familiar once you look for them: fatigue that does not track with effort, irritability that surprises you, a narrowed range of feeling, intrusive sadness, sleep that does not restore.
For professional caregivers there is one additional move: watch the detachment that started as protection. The moment it begins to harden into something else, that is a signal to slow the caseload or to seek supervision, not to push harder. Compassion fatigue does not announce itself. It arrives as quiet cynicism, then as numbness, then as a version of you that no longer feels anything in the room.
What it looks like further in
Caregiver burnout is particularly cruel in its later stages because the symptoms turn against the relationship that produced them. The classic burnout signature, exhaustion sleep does not touch, helplessness, the sense that nothing you do matters, arrives here on top of love or vocation. The cynicism does not stay clean and external. It seeps inward. You start resenting the person you are caring for. You catch yourself going through motions for someone you used to feel fierce protectiveness toward. For professional caregivers it is the same shape: the patient becomes a case number, the client becomes an interruption, and the version of you that chose this work no longer arrives in the room.
That is the part most people are not warned about. It is also, mercifully, reversible. The earlier the loop is named, the easier it is to interrupt. Naming it does not make the load any lighter. It makes it possible to ask for the supervision, the respite, the grief work that this kind of burnout actually responds to, instead of pushing harder out of guilt, which is the move that drives the loop deeper.
Where this is, and where it isn’t
There is one more obstacle, especially for caregivers who are not professionals. The internal rule is often unspoken but absolute: I must not feel this. This is my paramount duty. Naming yourself as overloaded by work is socially permitted. Naming yourself as overloaded by caring for your own child, or your own parent, sounds close to monstrous from the inside, so the words do not get said, even silently. But that admission is precisely where the work begins.
You cannot recover from a burnout you are not allowed to have.
One question is usually enough: is the load yours, or are you carrying it for someone else?
If the load is work you could in principle reduce, you are probably in one of the other types. If the load is another human being whose situation you cannot accelerate or interrupt, this episode is yours. The recovery path is different, and the first honest move is to stop trying to apply advice built for a problem you do not have.
What is coming in the next episodes?
Next — NL B5: Misalignment burnout. When the role fits you, but what the role is being used for does not. Reducing hours does not reduce the friction, because the friction is not about volume. It is about what you are spending your skill on.